Patients with severe mood disorders tend to respond more favorably to electroconvulsive therapy (ECT) when electrode placement has been individually selected for them. Yet most ECT practitioners use one electrode placement—bitemporal—for all patients (Figure 1).1
While standard bitemporal ECT is generally most effective, it also produces the greatest degree of disorientation, which can prolong a hospital stay or increase the need for supportive care.
Bifrontal ECT (Figure 2, part A) has been shown as efficacious as bitemporal placement while producing less disorientation.2 I have found left anterior right temporal (LART) placement (Figure 2, part B), to be equally effective with fewer side effects.
Figure 1 Bitemporal electrode placement
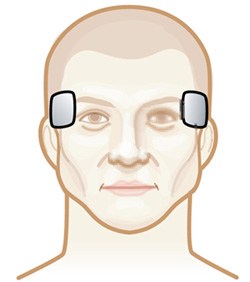
This generally effective and most widely used electrode placement causes the greatest post-ECT disorientation.
Figure 2a Bifrontal placement
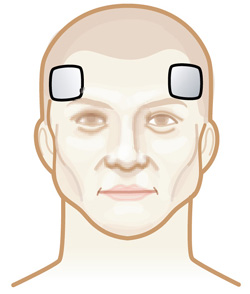
Figure 2b Left anterior right temporal (LART) placement
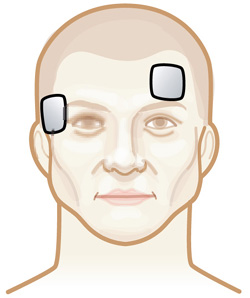
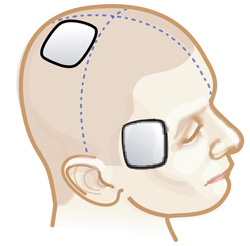
Figure 2c Right unilateral placement
Side Effects of Lart
Side effects such as disorientation and loss of self-care should be less severe and prevalent with LART than with other bilateral placements because:
- the left electrode is far anterior to the temporal lobe, rather than close to it as in bitemporal placement.
- LART avoids symmetrical effect, which can block compensation by the opposite hemisphere.
Hypothetically, some patients might not respond to bifrontal or LART placement but respond to bitemporal ECT, although no such instances have been reported in the literature. By contrast, response to bitemporal ECT after failure of right unilateral ECT (Figure 2, part C) is well known; indeed, studies of unilateral ECT typically include provisions for changing to bitemporal ECT. Moreover, early relapse (within 2 months) appears more frequently after unilateral ECT.
Patient Selection and Dosing
Low-dose right unilateral ECT should suffice in men younger than age 40 because they usually develop vigorous seizures without substantial disorientation afterward. Low dose in unilateral ECT is millicoulomb (mC) charge less than 4 times the patient’s age in years.
In patients who do not develop vigorous seizures—a common problem in men age >65—unilateral ECT is more likely to produce disappointing results than other ECT configurations. Moreover, severe confusion from unilateral ECT is not rare in patients older than 65. Unilateral ECT should not be a routine choice for this age group.
Stimulus dosing in effect alters electrode placement. High dose spreads the stimulus as if the electrodes were much larger. As a result, all forms of placement at high stimulus doses more closely resemble bitemporal ECT, increasing side effect risk and negating differences among the forms of electrode placement. In fact side effects from unilateral ECT at high stimulus doses approximate those of bitemporal ECT.3 Right unilateral ECT in this context has no apparent advantages.
When intervention with ECT is urgently needed—such as for patients with severe catatonia, inanition, or active suicidality—efficacy is paramount and bitemporal ECT is the usual choice. Typical starting dose in mC is 2.5 times age.
In nonemergency circumstances, my experience with LART placement has resulted in strong enthusiasm for ECT by nursing staff and patients who recognize improvement without noticeable side effects.
Clinicians who use ECT should obtain first-hand experience with all four methods of electrode placement. In addition, use of brief-pulse rather than sine-wave stimuli is as important to minimizing side effects as electrode placement.
Disclosure
Dr. Swartz has equity interests in Somatics, LLC, a manufacturer of ECT instruments.