More than 50% of psychiatrists have experienced the death of a patient by suicide.1 For many of us, suicide represents the most feared outcome of a patient’s mental illness and makes managing suicide risk critical to everyday practice.
Unfortunately, we have little ability to predict suicide. Research into risk factors and the use of suicide rating scales have produced no consistently definitive methods to determine who will and who will not attempt or complete suicide.2 The purpose of suicide assessment, then, is not to predict suicide but to help us understand the sources of a patient’s suicidality and develop an informed intervention.
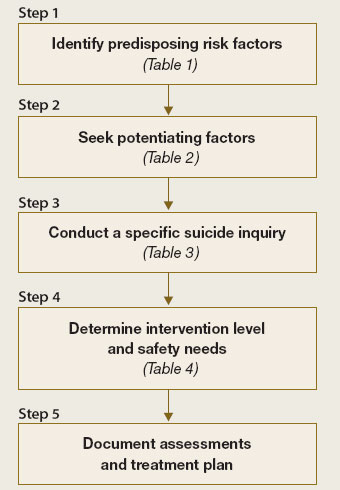
This article describes a practical, commonly accepted approach to suicide risk assessment and intervention, based on the B-SAFE model (Basic Suicide Assessment Five-step Evaluation) proposed by Jacobs et al (Figure).3 Using this method to assess suicide risk can help you answer questions such as:
- Which factors are most important to consider when evaluating suicide risk in my patient?
- What questions should I ask my patient to find out if he or she is suicidal?
- How do I know if a patient is at risk for suicide?
- What emergent interventions are called for when managing the acutely suicidal patient?
- How should I document a suicide risk assessment?
Figure Basic Suicide Assessment Five-step Evaluation (B-SAFE)
Source: Created from information in references 2,11
Why ask about suicide?
No single risk factor or combination of risk factors can predict or preclude suicide. Even so, attempting to evaluate an individual’s risk by asking about suicidal thinking, reviewing risk factors, or using clinical rating scales helps you determine the next appropriate action (discharge, medication, psychiatric referral, consultation, or hospitalization).
While talking to patients and evaluating their risk for suicide, you may begin to understand their suffering—described as the most common denominator in suicide2 and perhaps the most important clue to heightened suicide risk. Such an exploration allows you to identify potential:
- risk factors that can be modified
- preventative factors to promote.
Don’t be afraid to ask. Asking about suicidal thoughts is necessary—but not enough—to understand an individual’s potential for suicide. Never be afraid to ask patients about suicide, believing that doing so will “put ideas into their heads.” By the same token, a patient who denies thoughts or plans for suicide may still be at risk.
Identifying at-risk patients is much more difficult than just asking if they are considering suicide. Opening a concerned dialogue can provide a sense of relief to the patient while allowing you to explore:
- the extent and seriousness of the suicidal thoughts
- associated risk factors or conditions, such as depression.
Stepwise risk assessment
The first 3 steps of Jacobs’ B-SAFE model focus on identifying predisposing and protective factors for suicide.3 For an in-depth discussion, consult the American Psychiatric Association practice guideline for the assessment and treatment of patients with suicidal behaviors4 (available at http://www.psych.org/psych_pract/treatg/pg/suicidalbehavior_05-15-06.pdf).
STEP 1: Risk factors. Use the patient interview, medical records, and collateral information to uncover potential suicide risk factors (Table 1).2
Psychopathology. Focus on depression, bipolar disorder, schizophrenia, substance abuse, and personality disorders, which are strongly associated with suicide. These disorders are considered modifiable risk factors—diagnosis and appropriate treatment can diminish suicide risk.
Suicidality has been associated with early depression or bipolar disorder, often before patients receive a diagnosis or effective treatment. Recovery and immediate post-discharge periods also are thought to be times of heightened suicide risk.
Psychosocial variables. Demographic and psychosocial variables may influence suicide risk estimation. A retrospective study of 100 patients who attempted suicide suggests that the most predictive factors for suicide are:
- living alone
- being aged 17 to 35 (although in other studies, more advanced age also has been linked to increased suicide risk3)
- complaints of severe hopelessness, anhedonia, and insomnia.5
Physical illness may potentiate suicide risk. Medical illnesses that produce great pain, disfigurement, limited function, or fear of dependence may reduce a person’s will to live and increase suicide risk.6 Epilepsy has been associated with a 4- to 5-fold increase in suicide risk7 and is the only medical diagnosis to carry a documented increase in suicide among children and adolescents.8 Often these medical disorders coexist with psychiatric disorders, complicating the task of determining independent risk.
Severity of attempts or self-mutilation. When evaluating self-injurious or suicidal behavior in the emergency setting, consider the severity of the attempt as part of overall suicide assessment. Self-injurious behavior (cutting or burning) or impulsive suicide attempts (planned for <3 hours, committed in the presence others, or where discovery is very probable) appear to carry less severity or intent to die than do carefully planned and/or hidden suicide attempts.9 However, consider at high risk for suicide any patient with self-mutilating or suicidal behavior who expresses persistent intent to die; acute stabilization on an in-patient unit may be necessary.