Dr. Hillard states that “light therapy should not be used without pharmacotherapy to treat a major depressive episode” in seasonal affective disorder, or SAD (Current Psychiatry, December 2002).
It is well supported that both full syndromal and sub-syndromal winter depression can be successfully treated with light therapy alone.1,2 Response rates have varied between 60 and 90%. Many—if not most—SAD specialists consider light therapy the treatment of choice.1 Antidepressant medication can be added later if light therapy does not achieve an optimal result.
An error appeared in Figure 1 of the Current Psychiatry supplement, “Foundational treatment for bipolar disorder” (March 2003). The correct figure is printed here.
Figure 1 Antimanic efficacy of olanzapine, 15 mg/d, in acute bipolar mania and mixed episodes
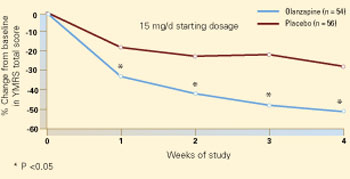
Patients with acute bipolar mania or a mixed episode were treated with olanzapine or placebo for 4 weeks in a randomized, double-blind trial. Compared with placebo, olanzapine at a starting dosage of 15 mg/d was associated with significant symptom improvement in the first week (50% change from baseline in Young Mania Rating Scale total score). This trend continued throughout the trial.
Source: Reprinted with permission from Tohen M et al. Arch Gen Psychiatry 2002; 57(9):841-9. Copyright 2002. American Medical Association
Psychotropics are first-line therapy only for severely depressed inpatients with SAD.2 This occurs infrequently, however, and even in these rare cases the efficacy of drug vs. light therapy or combined treatment has not been definitively studied.
J. Daniel Kanofsky MD, MPH; Assistant professor of psychiatry
Albert Einstein College of Medicine of Yeshiva University; Bronx, NY
Brenda Byrne, PhD; Margolis Berman Byrne Health Psychology Philadelphia, PA
- Wirz-Justice A. Beginning to see the light. Arch Gen Psychiatry 1998;55(10):861–2.
- Lam RW. Seasonal affective disorder: diagnosis and management. Primary Care Psychiatry 1998;4:63-74.
Your article on SAD indicates that “Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously well-controlled depressive symptoms worsen in the fall or winter.”
However, Philips Electronics states on its Web site: “Do not take antidepressants in combination with light therapy—this may damage your eyes.”1
I would like an authoritative, reliable resolution. Can light therapy be used concurrently with antidepressants without resulting in eye damage?
Martin Schwartz; New York, NY
- Philips Bright Light Energy: Alternatives to light baths. Available at: www.brightlight.philips.co.uk/b/4.html. Accessed Feb. 25, 2003.
Dr. Hillard responds
I thank Drs. Kanofsky and Byrne and Mr. Schwartz for their insights.
After an extensive search of the literature and the Philips Electronics Web site, we can find no justification for not using drug therapy in SAD.
J. Randolph Hillard, MD
Editor-in-chief