Three keys can help you safely treat dementia’s difficult behavioral and psychological symptoms:
- Differentiate medical from psychiatric causes of patients’ distress.
- Use antipsychotics and other drugs as adjuncts to psychosocial treatments.
- Start low and go slow when titrating dosages.
Although no treatment reverses the pathophysiology of progressive neurodegenerative disorders, managing agitation and other behaviors can alleviate patient suffering and reduce caregiver stress. Based on the evidence and our experience, this article describes a practical approach, including a treatment algorithm and evidence of atypical antipsychotics’ efficacy and side effects in this patient population.
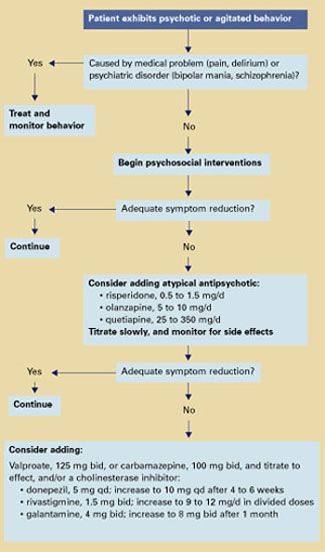
Algorithm Treating behavioral symptoms in patients with dementia
Dementia’s behavioral symptoms
An International Psychogeriatric Association consensus statement1 grouped dementia’s behavioral and psychological symptoms into two types:
- those usually assessed by interviewing patients and relatives—anxiety, depressed mood, hallucinations, and delusions
- those usually identified by observing patient behavior—aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviors, sexual disinhibition, hoarding, cursing, and shadowing.
These behaviors in community-living patients are distressing to family members and increase the risk for caregiver burnout—the most common reason for placing older patients in long-term care. In the nursing home, dementia’s symptoms reduce patients’ quality of life; interfere with feeding, bathing, and dressing; and—when violent—may endanger staff and other patients.
Rule out a medical cause
Differential diagnosis. Behavioral symptoms in dementia tend to be unpredictable, which makes diagnosis and treatment challenging. The first step is to determine if a medical or psychiatric condition might account for the behavior. For instance:
- A patient with dementia may be agitated because of a distended bladder or arthritis but unable to communicate his or her pain in words.
- In mild dementia, a pre-existing psychiatric disorder such as schizophrenia might be causing a patient’s hallucinations or delusions.
- Pacing and restlessness may be drug side effects and might be controlled by reducing dosages or switching to less-activating agents.
Delirium is also a risk for older patients—especially those with degenerative neurologic disorders. Common triggers in older patients include acute illness such as a urinary tract infection or pneumonia, alcohol or benzodiazepine withdrawal, anticholinergic agents, medication changes, and dehydration.
Delirium is characterized by acute onset and fluctuating neuropsychiatric symptoms, including disturbed consciousness and changes in attention and cognition. Taking a careful history to learn the course of treatment and the patient’s baseline cognitive function can help you differentiate dementia from delirium. Family members, physicians, and nursing staff are valuable sources of this information.
Use antipsychotics as adjuncts
Psychosocial interventions. After medical causes have been ruled out, consensus guidelines2 recommend psychosocial interventions as first-line treatment of dementia’s behavioral symptoms (Algorithm). Suggested interventions for patients and caregivers are listed in Table 1.3
Antipsychotics. For patients who respond inadequately to psychosocial measures, the next step is to add an atypical antipsychotic. Because of side effects, conventional antipsychotics are not recommended for patients with dementia.
When prescribing atypicals, remember that older adults:
- are more sensitive to side effects than younger adults
- require lower starting and target dosages
- exhibit heterogeneity of response.
Older patients’ medical status can range from “fit” to “frail,” which influences individual response to medications. Generally, age-related changes in the way their bodies metabolize drugs account for older patients’ increased sensitivity to drug side effects (Box).4-11
Atypical antipsychotics and dosages that have been shown benefit for managing behavioral symptoms in older patients with dementia include:
- risperidone, 0.5 to 1.5 mg/d12
- olanzapine, 5 to 10 mg/d13
- quetiapine, 25 to 350 mg/d14 (Table 2).15,16
Start with low dosages, and titrate slowly. Increase once or twice a week until the lowest effective dosage is reached.
Augmenting agents. If antipsychotic monotherapy fails to achieve an adequate response or if side effects limit dosing, adjunctive agents may be added with caution. Augmenting agents that have shown benefit in some patients with dementia include:
- mood stabilizers such as divalproex17 or carbamazepine18
- cholinesterase inhibitors, such as donepezil, rivastigmine, or galantamine.19
Start divalproex at 125 mg bid or carbamazepine at 100 mg bid and titrate to effect. Concomitant carbamazepine will decrease blood levels of risperidone, olanzapine, and quetiapine because of hepatic enzyme induction.20
Start donepezil at 5 mg once daily and increase after 4 to 6 weeks to 10 mg qd. When using rivastigmine, start with 1.5 mg bid and titrate to 9 to 12 mg/d in divided doses. Start galantamine at 4 mg bid and increase after 1 month to 8 mg bid.
Table 1
Suggested psychosocial interventions for older patients with dementia
Communicate clearly
|
Minimize the impact of sensory deficits
|
Modify environment when necessary
|
Encourage consistent daily routines
|
Optimize social/physical stimulation
|
Encourage caregiver to:
|