Mrs. M, 35, is undergoing breast cancer treatment. She is referred to the consultation-liaison service by an emergency room physician for evaluation of suicidal thoughts.
Mrs. M has been crying for 2 hours. She awoke this morning feeling that she could no longer deal with “the unknown.” She has lost her hair and 30 pounds during chemotherapy and hardly recognized herself in the bathroom mirror. She thought about killing herself until one of her children walked by. After they went to school, she drove to the emergency room.
When you ask if she has had other thoughts of hurting herself, she says, “I would never do anything like that to my family, but the fact that I was thinking about it really scared me.”
Each patient responds uniquely to the emotional trauma of having a chronic or life-threatening medical illness. Coping styles depend on medical, psychological, and social factors as well as the person’s personality and experiences. Reactions range from mature to psychotic.
To help you guide patients such as Mrs. M through difficult medical treatments and decisions, we describe:
- a psychiatric workup to identify maladaptive response to illness
- typical emotional and behavioral responses to chronic illness
- how to provide psychotherapy tailored to the needs of 7 personality styles of medically ill patients.
Psychiatric Workup
Mrs. M is married with 3 sons. She found a lump on her breast 4 months ago but decided to wait “because, I thought, ‘it can’t be anything bad; it will go away.’” When the lump remained 3 months later, she consulted a specialist who diagnosed breast cancer.
Mrs. M underwent a lumpectomy and has been receiving weekly chemotherapy. Besides losing her hair, she says she has no appetite. Looking at food or driving close to the hospital makes her nauseous. She starts vomiting before she arrives for chemotherapy.
Though her family supports and encourages her, she can’t stop thinking about death. She feels isolated, lonely, and cries often. “No one understands what I am going through,” she says. “How can I share these feelings with them?”
Physicians such as the specialist who diagnosed Mrs. M’s cancer often must communicate difficult information. Careful planning when delivering bad news (Box 1)1,2 can set the stage for a healthier emotional and behavioral response.
Chronic illness causes depression in up to 25% of patients.3 At particular risk of developing depressive symptoms are patients with:
- poor physical condition
- poorly controlled pain
- advanced illness
- history of major depressive disorder
- family history of depression and suicide
- certain cancers, such as of the pancreas, lung, head or neck.4
Mechanisms of depression in illness. Depression can be the first symptom of some medical illnesses, such as pancreatic or liver cancer. Diseases that directly affect the brain—such as Parkinson’s disease, multiple sclerosis, and systemic lupus erythematosus—can cause depression. Patients disabled by spinal cord injury, stroke, or cancer also are at risk for depression.
Treatment is the same, whether illness-related chemical changes or the patient’s emotional response to disability is causing the depression. When diagnosing depression in medically ill patients, DSM-IV-TR recommends using criteria for major depression and providing treatment, whatever the cause.
Mrs. M has trouble sharing feelings of hopelessness with her family. Her changes in demeanor and isolation from everyday activities are clues to clinical depression and anxiety.
Depression can be difficult to diagnose when medical illness causes depression-like symptoms.5 To make the diagnosis, ask patients with chronic illness about depression’s emotional symptoms (hopelessness, withdrawal from others, sadness, ruminating thoughts, frequent crying spells), rather than its physical symptoms of poor eating, disturbed sleep, or low energy that may stem from the medical illness. Patients might not be as hard on themselves if they feel the medical illness—not poor coping on their part—caused their depression.
Box 1 6 steps for delivering bad medical news
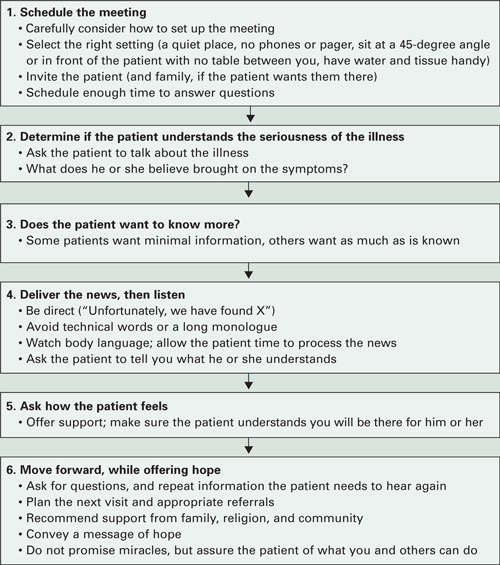
Source: Adapted from references 1, 2Workup. Our workup of Mrs. M includes thyroid function tests, CBC, comprehensive metabolic panel, and brain MRI to rule out metastasis. All are negative. In her history, Mrs. M reports a previous episode of major depression 5 years ago that was successfully treated with sertraline for 1 year.
Consistent with her workup and symptoms, we diagnose major depression without psychosis. Cancer patients who report hopelessness are at increased risk of suicide. Because of her family support and religious beliefs, however, we feel she can safely go home and return for follow-up the next week.
Emotional response to illness
Mrs. M starts weekly outpatient appointments at our clinic. Because sertraline has worked for her in the past, it is our first choice to increase her energy, improve her mood, and decrease her hopelessness. Initial dosage is 25 mg/d for the first 3 days, with an increase to 50 mg/d for 1 month, and 100 mg/d thereafter. She reports no side effects.