Case: 'He's okay on weekends'
Nathan, age 13, is referred by his parents for recent school refusal behavior. He has had difficulty adjusting to middle school and has been marked absent one-third of school days this academic year. These absences come in the form of tardiness, skipped classes, and full-day absences.
Nathan complains of headaches and stomachaches and says he feels upset and nervous while in school. His parents, however, complain that Nathan seems fine on weekends and holidays and seems to be embellishing symptoms to miss school. Nathan’s parents are concerned that their son may have some physical or mental condition that is preventing his school attendance and that might be remediated with medication.
Child-motivated refusal to attend school or remain in class an entire day is not uncommon, affecting 5% to 28% of youths at some time in their lives.1,2
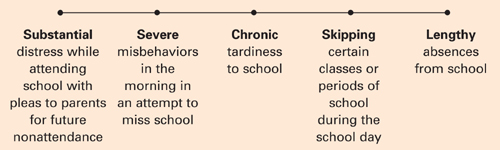
The behavior may be viewed along a spectrum of absenteeism (Figure), and a child may exhibit all forms of absenteeism at one time or another. In Nathan’s case, for example, he could be anxious during school on Monday, arrive late to school on Tuesday, skip afternoon classes on Wednesday, and fail to attend school completely on Thursday and Friday.
In this article you will learn characteristics of school refusal behavior to watch for and assess, and treatment strategies for youths ages 5 to 17. You will also find advice and techniques to offer parents.
Figure A child might exhibit each behavior on this spectrum at different times
Refusal behavior characteristics
School refusal behavior encompasses all subsets of problematic absenteeism, such as truancy, school phobia, and separation anxiety.3 Children and adolescents of all ages, boys and girls alike, can exhibit school refusal behavior. The most common age of onset is 10 to 13 years. Youths such as Nathan who are entering a school building for the first time—especially elementary and middle school—are at particular risk for school refusal behavior. Little information is available regarding ethnic differences, although school dropout rates for Hispanics are often considerably elevated compared with other ethnic groups.4,5
School refusal behavior covers a range of symptoms, diagnoses, somatic complaints, and medical conditions (Tables 1-3).6-12 Longitudinal studies indicate that school refusal behavior, if left unaddressed, can lead to serious short-term problems, such as distress, academic decline, alienation from peers, family conflict, and financial and legal consequences. Common long-term problems include school dropout, delinquent behaviors, economic deprivation, social isolation, marital problems, and difficulty maintaining employment. Approximately 52% of adolescents with school refusal behavior meet criteria for an anxiety, depressive, conduct-personality, or other psychiatric disorder later in life.13-16
Table 1
Common symptoms that could signal school refusal behavior
| Internalizing/covert symptoms | Externalizing/overt symptoms |
|---|---|
| Depression | Aggression |
| Fatigue/tiredness | Clinging to an adult |
| Fear and panic | Excessive reassurance-seeking behavior |
| General and social anxiety | Noncompliance and defiance |
| Self-consciousness | Refusal to move in the morning |
| Somatization | Running away from school or home |
| Worry | Temper tantrums and crying |
Table 2
Primary psychiatric disorders among youths with school refusal behavior
| Diagnosis | Percentage |
|---|---|
| None | 32.9% |
| Separation anxiety disorder | 22.4% |
| Generalized anxiety disorder | 10.5% |
| Oppositional defiant disorder | 8.4% |
| Major depression | 4.9% |
| Specific phobia | 4.2% |
| Social anxiety disorder | 3.5% |
| Conduct disorder | 2.8% |
| Attention deficit/hyperactivity disorder | 1.4% |
| Panic disorder | 1.4% |
| Enuresis | 0.7% |
| Posttraumatic stress disorder | 0.7% |
| Source: Reference 7 | |
Table 3
Somatic complaints and medical conditions
commonly associated with school refusal behavior
| Somatic complaints | Medical conditions |
|---|---|
| Diarrhea/irritable bowel | Allergic rhinitis |
| Fatigue | Asthma and respiratory illness |
| Headache and stomachache | Chronic pain and illness (notably cancer, Crohn’s disease, dyspepsia, hemophilia, chronic fatigue syndrome) |
| Nausea and vomiting | Diabetes |
| Palpitations and perspiration | Dysmenorrhea |
| Recurrent abdominal pain or other pain | Head louse infestation |
| Shaking or trembling | Influenza |
| Sleep problems | Orodental disease |
Finding a reason for school refusal
If a child has somatic complaints, you can expect to find that the child is:
- suffering from a true physical malady
- embellishing low-grade physical symptoms from stress or attention-seeking behavior
- reporting physical problems that have no medical basis.
A full medical examination is always recommended to rule out organic problems or to properly treat true medical conditions.
Four functions. If no medical condition is found, explore the reasons a particular child refuses school. A common model of conceptualizing school refusal behavior involves reinforcers:1,2
- to avoid school-based stimuli that provoke a sense of negative affectivity, or combined anxiety and depression; examples of key stimuli include teachers, peers, bus, cafeteria, classroom, and transitions between classes
- to escape aversive social or evaluative situations such as conversing or otherwise interacting with others or performing before others as in class presentations
- to pursue attention from significant others, such as wanting to stay home or go to work with parents
- to pursue tangible reinforcers outside of school, such as sleeping late, watching television, playing with friends, or engaging in delinquent behavior or substance use.
The first 2 functions are maintained by negative reinforcement or a desire to leave anxiety-provoking stimuli. The latter 2 functions are maintained by positive reinforcement, or a desire to pursue rewards outside of school. Youths may also refuse school for a combination of these reasons.17 In Nathan’s case, he was initially anxious about school in general (the first function). After his parents allowed him to stay home for a few days, however, he was refusing school to enjoy fun activities such as video games at home (the last function).