It might seem business as usual in clinical psychiatry, but major transformative changes in the scientific foundation of the specialty are taking place. The “neuroscientification” of psychiatry, ongoing for more than 3 decades, is now approaching a tipping point: The specialty is on the verge of an unprecedented denouement of the old tenets and assumptions. Just as smartphones have made a 25-volume encyclopedia set obsolete, coming changes in scientific psychiatry will be fully disruptive to your father’s practice of psychiatry.
That situation will change, soon—as surely as medieval times gave way to the Renaissance. Psychiatry of the future will be drastically different once new models of objective diagnostic tests and physiologically specific interventions emerge from fast-moving discoveries of the molecular biology of the mind and its pathologies.
Most psychiatric practitioners do not regularly read neuroscience journals that describe the accelerating progress in molecular psychiatry, where the text is replete with an alphabet soup of terminology that one day will permeate the medical practice of the new psychiatry.
There are many reasons to be optimistic that transcendent scientific transformations will sweep away the fuzzy biologic, diagnostic, and therapeutic ambiguities that have plagued psychiatry for so long—plagued us because of the herculean challenges of investigating the divinely complex brain and its gloriously enigmatic mind. New methods and tools for exploration and paradigmatic shifts in conceptualizing the etiopathogenesis of psychiatric brain disorders are rapidly leading to a discarding of many simplistic, even primitive, notions that have guided psychiatry over the past century. Psychopharmacological breakthroughs of the past 50 years, which, admittedly, have yet to cure or eliminate disabilities associated with major psychiatric disorders, are only a prologue to the coming revolution in neuropsychiatry, in which prevention, not just intervention, will change everything. Curing deteriorative brain disorders will be a reality once that revolution in neuroscience enters its propitious translational phase.
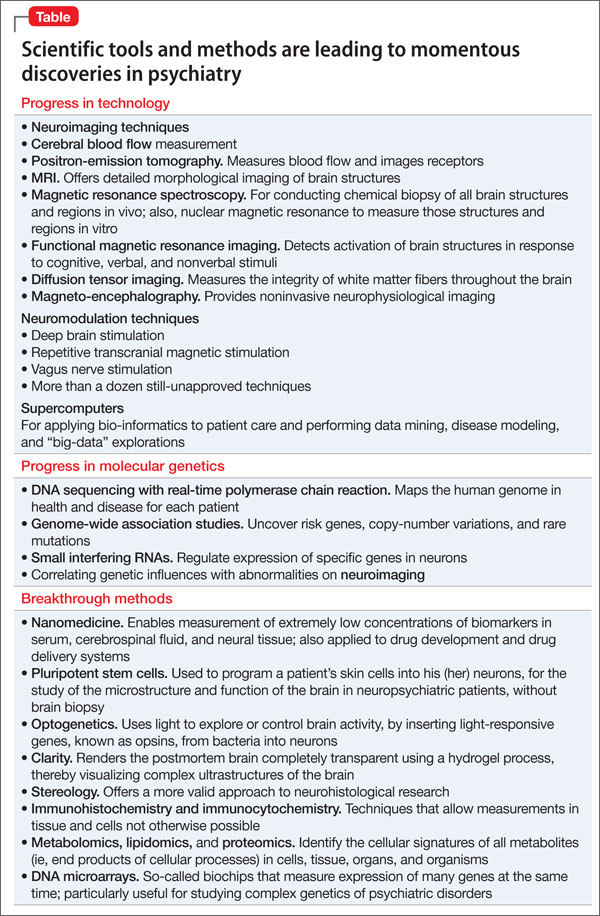
The Table presents a sampling of scientific progress that is setting the stage for disruptive technologies and probes that will lead to far more advanced diagnosis, prevention, and treatment of neuropsychiatric diseases.
We psychiatrists must keep up, regularly reading the latest literature to learn about the latest advances and to make sure we are familiar with the emerging language of psychiatric neuroscience. Instead of remaining fondly attached to ancient constructs such as id, ego, superego, and defense mechanisms, we should be thinking about the default mode network, seeking to understand the connectome, the envirome, the metabolome, and the proteome; microglial activation, inflammatory markers, IL-6, TNF alpha, oxidative and nitrosative stress, and physiologic vs pathologic apoptosis; BDNF, FGF, VEGF, MIF, GFAP, and S100B; neuroplasticity and dendritic spines; and genes such as CLOCK, NOTCH3, and Met-to-Val mutations—and so on.
Those of us who do not adapt to swift transition of knowledge might suffer the fate of clinical dinosaurs, as the massive asteroid of neuroscientific advances smashes into the placid landscape of psychiatry. As Alvin Toffler, author of Future Shock, proposed, the illiterates of the future will not be the people who cannot read or write. They will be the ones who fail to learn.